- Home
- About the Journal
- Peer Review
- Editorial Board
- For Authors
- Reviewer Recognition
- Archive
- Contact
- Impressum
- EWG e.V.
Cite as: Archiv EuroMedica. 2022. 12; 4: e1. DOI 10.35630/2199-885X/2022/12/4.12
One of the current problems of modern obstetrics is the diagnosis, treatment and prevention of intrauterine growth retardation. This pathology ranks second after prematurity among the causes of low-birth-weight babies. The prevalence of fetal retardation varies worldwide from 6.5 to 30.0% of all births, of which about 23% are very low birthweight and about 38% extremely low birthweight babies. A new coronavirus infection, caused by the viral pathogen SARS-CoV-2, which contributes to thrombotic microangiopathy in combination with hypercoagulation syndrome, is currently ongoing. During physiological pregnancy, there is known to be an increased risk of complications associated with both bleeding and thrombosis, which are affected by changes in fibrinolytic activity and hypercoagulable state, endothelial dysfunction, and changes in blood rheological properties. It significantly increases the risk of pregnancy complications such as pre-eclampsia, placental insufficiency, fetal hypoxia, and therefore leads to intrauterine growth retardation of the fetus. This study analyzed the status of newborn babies and the incidence of intrauterine growth retardation in women who had contracted coronavirus infection. Two groups of women were included in study: the first included those who became pregnant 3 to 6 months after a new coronavirus infection, and the second was a control group. The study found that women in the first group were more likely to have pre-eclampsia and their babies were more likely to be diagnosed with intrauterine growth retardation.
Keywords: intrauterine growth retardation, coronovirus infection, pregnancy, thrombotic microangiopathy, newborns.
One of the current problems of modern obstetrics is the diagnosis, treatment and prevention of intrauterine growth retardation (IUGR). This pathology ranks second after prematurity among the causes of low birth weight. The prevalence of fetal retardation varies worldwide from 6.5-30.0% of all births, of which about 23% are very low birthweight and about 38% extremely low birthweight. VTE contributes to high rates of morbidity and mortality in preterm infants. [1,2].
Observation of patients with COVID-19 revealed that the course of the disease is accompanied by thrombotic microangiopathy combined with hypercoagulable syndrome. These are based on endothelial cell dysfunction, provoked both directly by the virus and by the cytokine storm that develops, and subsequently by autoimmune damage. [3,4].
It is known that during physiological pregnancy there is an increased risk of complications associated with both bleeding and thrombosis, which is affected by changes in fibrinolytic activity and a state of hypercoagulation, endothelial dysfunction, and changes in blood rheological properties [5]. The overlap of these changes with thrombotic microangiopathy as a result of a new coronavirus infection can significantly increase the risk of pregnancy complications such as pre-eclampsia, placental insufficiency, fetal hypoxia and, consequently, lead to intrauterine growth delay, making this study relevant. (6,7).
The aim of this study was to analyze the status of the newborn babies of patients who had coronavirus infection and to identify the relationship between coronavirus infection and the development of IUGR.
To examine the effect of new-onset coronavirus infection on the newborns, 55 patients (CI group) aged 22-32 years who had a desired pregnancy from 3 to 6 months after a new coronavirus infection (n=55) and 28 patients (CII group) who had not had COVID-19 (n=28) were examined. Group CII pregnant women were divided into three subgroups depending on the severity of the disease they had suffered: mild (n=15), moderate (n=22) and severe (n=18). In mild disease, clinical symptoms were limited to subfebrile fever, weakness, general malaise, cough, and sore throat. At intermediate severity, body temperature rose above 38°C, respiratory rate over 22 per minute, dyspnea on exercise, characteristic changes on CT or chest radiography, a drop in saturation below 95%, an increase in serum C-reactive protein over 10 mg/l. In the severe course, unstable hemodynamics with fall of arterial pressure, decreased consciousness, marked changes in the lungs on tomograms or radiographs typical of viral lesions, respiratory rate over 30 per minute, oxygen saturation falling below 93%, PaO2 to FiO2 ratio below 300 mmHg, arterial blood lactate over 2 mmol/L, and qSOFA over 2. Patients in this subgroup received comprehensive inpatient treatment.
On collection of anamnesis and initial examination it was found that concomitant somatic pathology was noted in 95.1% of pregnant women. The predominant nosological form was chronic iron deficiency anemia (56.6%), followed by thyroid disease (27.7%), followed by visual disorders (21.6%) and gastrointestinal diseases (14.4%).
Concomitant gynecological diseases were detected in one third of pregnant women. Cervical ectopy predominated among the nosological forms (16.8%), ovarian cysts came second (4.8%), and chronic adnexitis came third (2.4%).
Parity analysis showed that most of the patients were first-pregnant and first-time mothers, one third of the women interviewed were repeat-pregnant, and 25.3% of the women were second-pregnant. A 14.4% of the patients were found to have a history of obstetric complications.
Analysis of the clinical course of pregnancy showed that the chief complication was early toxemia manifested by nausea, vomiting, excessive salivation and accompanied by drowsiness, irritability, weakness, decreased appetite, intolerance to smells and affecting 27.7% of the total number of patients surveyed. The threat of spontaneous miscarriage in the first trimester was noted in 4.8% of patients as a sense of discomfort and/or mild heaviness, aching or aching pain in the lower abdomen, which increased with physical activity, in some pregnant women with irradiation to the lumbar and/or sacral regions. No statistically significant difference was found between the groups.
In the second trimester, threat of spontaneous miscarriage was recorded in 12% of pregnant women. The threat of miscarriage was manifested by tensive or aching pains in the lower abdomen, in some cases accompanied by bloody discharge; persistent or recurrent uterine hypertonicity on objective obstetric and ultrasound examinations; and the development of isthmic-cesmic insufficiency.
In the early second trimester, the following preclinical signs of pre-eclampsia were noted: a positive reversal test (change in diastolic blood pressure of more than 20 mmHg at 5-minute intervals when the pregnant woman was initially lying on her side and then on her back and then on her side again); no reduction in SBP in the spiral arteries of the myometrium and uterine arteries at 14-16 weeks' gestation on Doppler ultrasound, indicating impaired uterine-placental blood flow; lower platelet count (less than 160x109/l), which progressively increases with gestational age; lymphopenia (18% or less); a decrease of PATT below 20 sec, platelet aggregation as high as 76%, hyperfibrinogenemia up to 4.5 g/l, indicating hypercoagulation in the cellular and plasma hemostatic components; decreased anticoagulant levels (endogenous heparin down to 0.07 units/ml. ml, antithrombin III up to 63%).
Clinical symptoms of pre-eclampsia were found in 10.8% of pregnant women: edema of the lower extremities, appearance of protein in the urinalysis, increased blood pressure, often accompanied by complaints of headache, dizziness, deterioration of well-being, weakness. The incidence of gestosis in the CI group was found to be 52.4% higher (p=0.56) than in the control group. It was found that severe COVID-19 patients had 2.1 times more often (p=0.56) manifestations of gestosis compared to those who had a mild illness, and 1.2 times more often (p=0.71) compared to those with a moderate degree of severity.
Signs of placental insufficiency were found in 12% of pregnant women. Its incidence was 86.9% higher in the CI group (p=0.28) compared to the control group. In patients with severe COVID-19 manifestations of placental insufficiency were 2.1-fold (p=0.56) more common compared to those with mild COVID-19 and 1.53-fold (p=0.77) compared to those with moderate COVID-19.
In the third trimester the threat of preterm birth was noted in 22.8%. Preeclampsia was detected in 10.8% of pregnant women. The most common clinical signs of pre-eclampsia were headache of different localisation, and the pregnant women complained of visual impairment, somnolence, mood swings, nausea, occasional vomiting, fever, and difficulty in breathing. Facial hyperaemia, tachypnoea, speech difficulties, hyperthermia and hearing loss were noted.
It was found that among the newborn babies 54.2% were boys and 45.8% were girls. It was found that babies of those women who had had a new onset of severe coronavirus infection prior to pregnancy were at their lowest weight: 9.4% (p=0.67) compared with babies of women who had a mild infection, and 5.3% (p=0.85) in the moderate degree, and 8.8% compared with the control group. In the same subgroup, there were 4 cases of prematurity out of 6 recorded in the study, 2 cases of fetal hypotrophy with intrauterine delay syndrome out of 4, and 2 cases of morpho-functional immaturity out of 3 (Table 1).
Table 1 The state of newborns in the examined puerperas (abs./%)
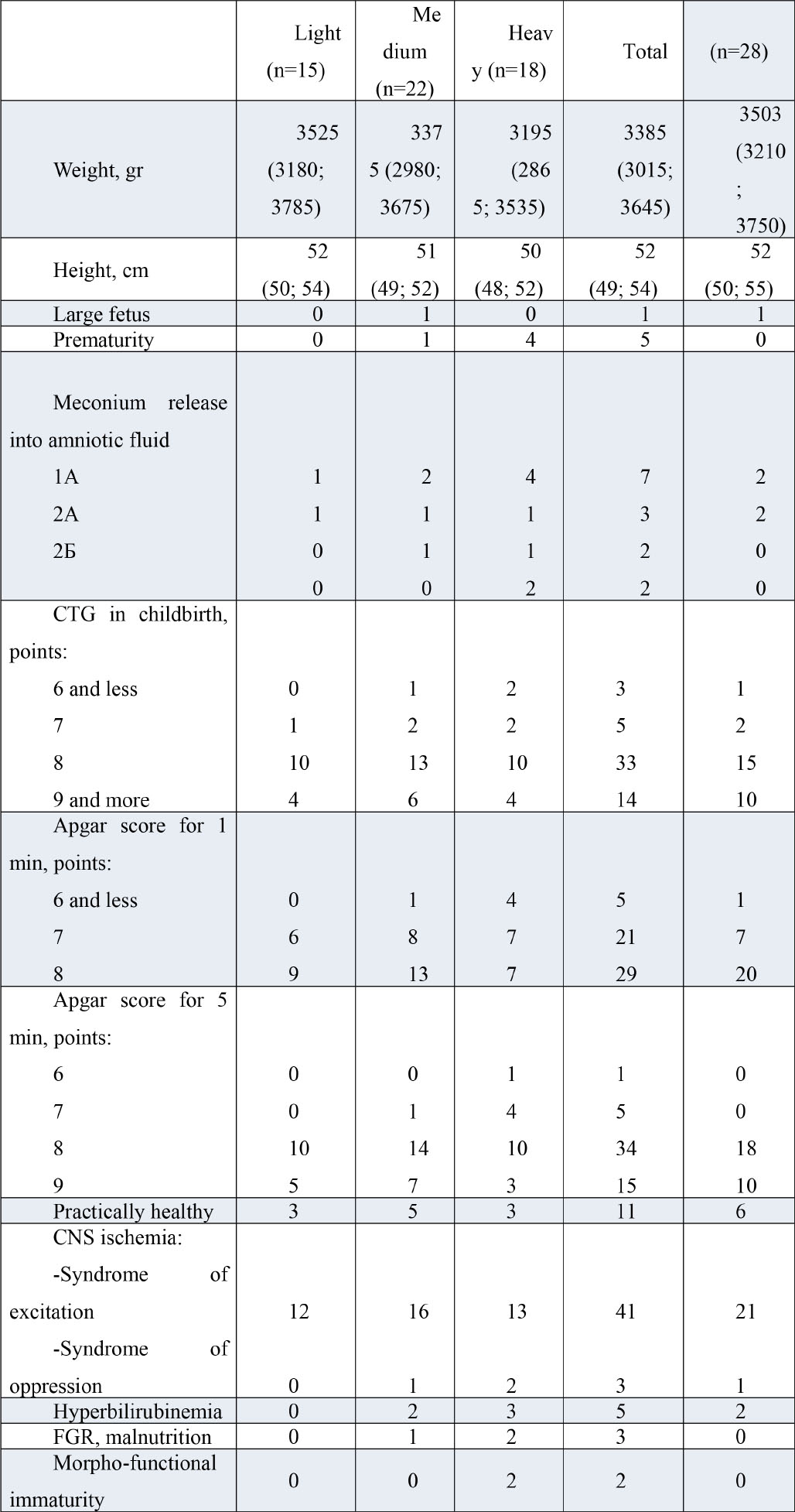
Meconium discharge into amniotic fluid was observed in 9 (10.8%) cases: including 5 cases of grade 1A, 2 cases of grade 2A and 2 cases of grade 2B. The CTG findings in labor in 4 (4.8%) cases were rated as 6, in 7 (8.4%) as 7, in 48 (57.8%) as 8, and in 24 (28.9%) as 9 or more. Although there were no statistical differences between the groups, there were 1.5 times more cases with a low score (6 or less) in group CI (p=0.99) than in the control group, and 28.6% fewer cases with a high score (9 or more), respectively (p=0.33). Apgar score of 6 on the Apgar scale at 1 minute was given to 6 babies (7.2%), 7 to 28 (33.7%), and 8 to 49 (59.0%). The number of babies with low scores (6 points) was 2.5 times (p=0.66) higher in group CI compared to group CII, and those with high scores (9 points or more) were 26.2% lower (p=0.16) respectively. At 5 minutes Apgar score of 6 was given to 1 neonate (1.2%), 7 to 5 (6.0%), 8 to 52 (62.6%), 9 to 25 (30.1%). The lowest scores were found in newborns in the subgroup of women who had had a severe new coronavirus infection, although overall no statistically significant differences were found.
Seventeen neonates (20.4% of the total) were found to be practically healthy. The rest had signs of central nervous system ischemia, including 4 (4.8%) with depression syndrome. Hyperbilirubinemia was noted in 7 children (8.4%).
Antenatal weight, as well as anthropometric parameters of newborns did not statistically significantly differ between the groups, but in the CI group it was 2.4% (p=0.97) lower than in the CII group. Perinatal weight was lowest in the subgroup of women with severe newborn coronavirus infection, as were the anthropometric parameters, with 9.5% (p=0.56) less than in the mild disease subgroup and 7.3% (p=0.72) less than in the moderate disease subgroup.
The fetal-placental ratio was not statistically significantly different between the groups, but its highest rate was found in the subgroup of women giving birth to COVID-19 in a severe degree: by 8.3% compared with the control group (p=0.63) and the subgroup with a mild course of the disease (p=0.64).
Structural and functional disorders of the placental microcirculatory bed, initially resulting from changes in the hemostasis system, are subsequently the cause of impaired growth and development of the fetus and cause immunological mechanisms of damage to placental structures. At research of placenta it is established, that in half of cases placental structure corresponded to gestational age, in 23 cases (27,7%) dissociated placental maturation, in 12 (14,4%) - delayed, in 2 (2,4%) - premature and in 2 (2,4%) - immaturity of placenta was marked. Among the morphological changes, calcinates in the placenta predominated - 30 (36.1%), followed by fibrinoid deposits in the stroma of villi and intervillous space - 28 (33.7%), moderate angiomatosis - 23 (27.7%), the fourth - signs of mild obliterating angiopathy - 19 (22.8%). In isolated cases, predominantly in the CI group, there were aphasic areas, haemorrhages, serous basal deciductitis, chorioamnionitis. It is noteworthy that the greatest changes in the placenta were seen in women who had a severe new coronavirus infection. Hypercoagulation syndrome, which is more common in this category of patients, can lead to increased fibrin deposition in the placenta and its premature ageing, increased vascular resistance and impaired uteroplacental blood flow.
Coronovirus infection, which predisposes to the development of haemostasis disorders during pregnancy, may contribute to an increased risk of complications such as gestosis, placental insufficiency, and fetal hypoxia accompanied by hypotrophy and intrauterine growth retardation syndrome. An inverse association has been found between the weight of babies born to women who have had coronavirus infection and the severity of the disease (the greater the severity of the disease, the lower the birth weight of the babies). Babies born to women with a coronavirus infection are more likely to have lower Apgar scores. The placenta of women with severe new-onset coronavirus infection has the greatest morpho-functional changes.
Kuneshko N.F.—literature review, text writing; Golomazova V.A. - collection and processing of materials, Gavrikova D.I. - statistical data processing; Kim V.V. - concept and design of the study, Pitirimova O.A. - critical revision of the article.
The authors declare the absence of obvious and potential conflicts of interest related to the publication of this article.
The authors state that there is no funding for the study.

|
||